
PATIENT PRESENTATION
A man in his mid-50s presented with a nonhealing right fifth toe amputation site. His risk factors included active smoking, diabetes, end-stage renal disease, hyper- lipidemia, and atrial fibrillation. He is maintained on 75 mg clopidogrel once daily and 5 mg apixaban twice daily. Noninvasive studies demonstrated patent femoropopliteal outflow with blunted ankle waveforms and noncompressible ankle-brachial indices (ABIs).
INTERVENTION
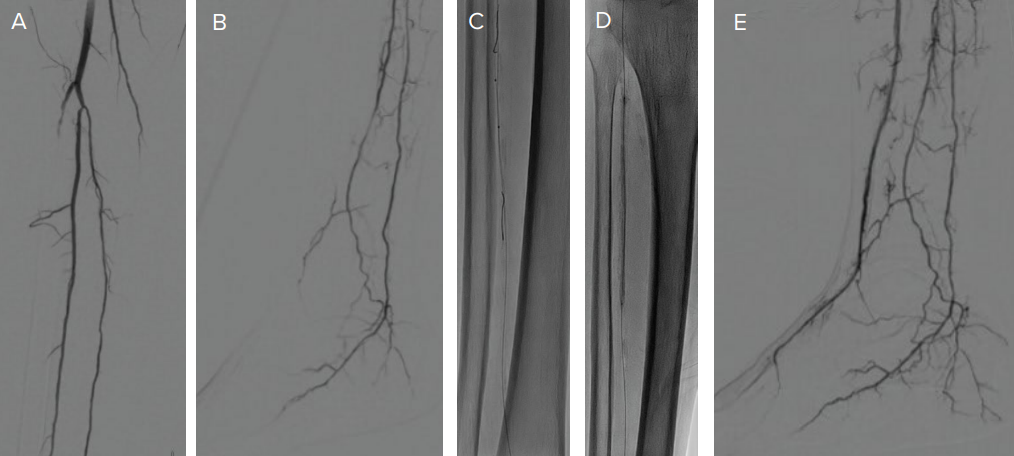
The procedure began with antegrade common femoral artery access with a 6-F, 25-cm sheath. Arteriography demonstrated patent peroneal and posterior tibial arteries with a long-segment chronic total occlusion (CTO) of the anterior tibial (AT) artery, which could not be recanalized from an antegrade approach (Figure 1A). There was a lack of flow in the dorsalis pedis (DP) artery to supply the target angio- some (Figure 1B). Retrograde access was obtained through a hibernating distal DP to facilitate AT recanalization using the subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) technique (Figured 1C). After predilation with a 2- X 40-mm balloon, a 3- X 120-mm Serranator PTA balloon was inflated slowly to 6
atm for 2 minutes over several stations from the DP to the proximal AT (Figure 1D). Completion arteriography demonstrated a widely patent AT and DP with perfusion to the target digit five wound bed (Figure 1E).
CONCLUSIONS
The Serranator balloon was perfectly suited to augment long-segment AT recanalization, achieving impressive luminal gain and brisk flow to the lateral forefoot wound. The patient went on to heal his minor amputation site wound in 6 weeks.
Are these results described in your cases typical for CLTI interventions?
Drs. Zimmermann and Leung: Satisfactory angiographic results are not consistently obtained with POBA alone despite meticulous sizing and prolonged inflation times. In our experience, serrated balloon angioplasty delivers consistently good results with decreased rates of flow-limiting dissection and vessel recoil compared to POBA, especially when treating heavily diseased BTK lesions, thus reducing the need for bailout stenting.
What is your inflation technique?
Drs. Zimmermann and Leung: Like with many endovascular devices, “go slow to finish fast.” With slow, controlled inflation, lesions will typically open well under nominal balloon pressure.
Why have you added the Serranator PTA balloon into your treatment algorithm?
Drs. Zimmermann and Leung: The Serranator PTA balloon fills a gap in the BTK treatment that was lacking with POBA alone. We’ve experienced consistently good results in terms of luminal gain and distal perfusion with a decreased need for post balloon scaffold placement. With its unique mechanism of action, the available Serranator PTA is well suited for the various BTK lesion morphologies encountered in CLTI patients and would likely be suitable for vessel prep before drug-coated balloon angioplasty.
