
Case StudiesBTK Revascularization in Patient with Gangrenous Wounds
Bradley Trinidad, MD | Northwest Physicians Group - Amarillo, TX
PATIENT PRESENTATION
A man in his mid-50s with coronary artery disease, diabetes, hypertension, peripheral vascular disease, and a history of smoking presented for evaluation of gangrenous changes to a right fifth toe amputation site performed by a podiatrist (Figure 1). He had a previous left BTK amputation at a neighboring hospital secondary to diabetic foot gangrene. Noninvasive studies were performed, revealing falsely elevated ankle-brachial index (ABI) secondary to medial calcinosis and toe pressure consistent with inadequate perfusion for wound healing. An arterial duplex ultrasound (DUS) indicated blunted monophasic waveforms of all three tibial vessels.

Figure 1. Gangrene of right fifth toe amputation site.
PROCEDURE DETAILS
After sterile draping, the right common femoral artery (CFA) was percutaneously accessed using ultrasound guidance and the micropuncture technique. After exchanging for a 5-F short sheath over a Glidewire Advantage guidewire (Terumo Interventional Systems), diagnostic angiography was performed. This revealed diffuse tibial vessel disease, with heavily calcified subtotal occlusions of the posterior tibial (PT) artery, anterior tibial (AT) artery, and tibioperoneal trunk (TPT). There was a notable midsegment occlusion of the AT artery, as well as occlusion of the dorsalis pedis artery (DPA; Figure 2). A 6-F, 45-cm Destination guiding sheath (Terumo Interventional Systems) was exchanged over the Glidewire Advantage into the distal popliteal artery. The patient was heparinized.
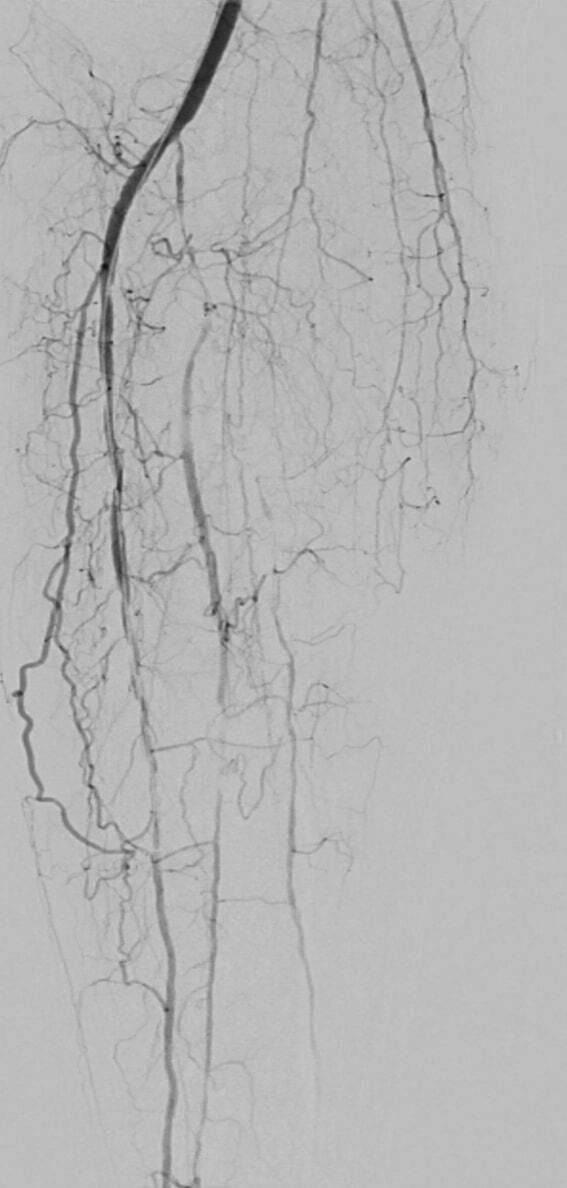
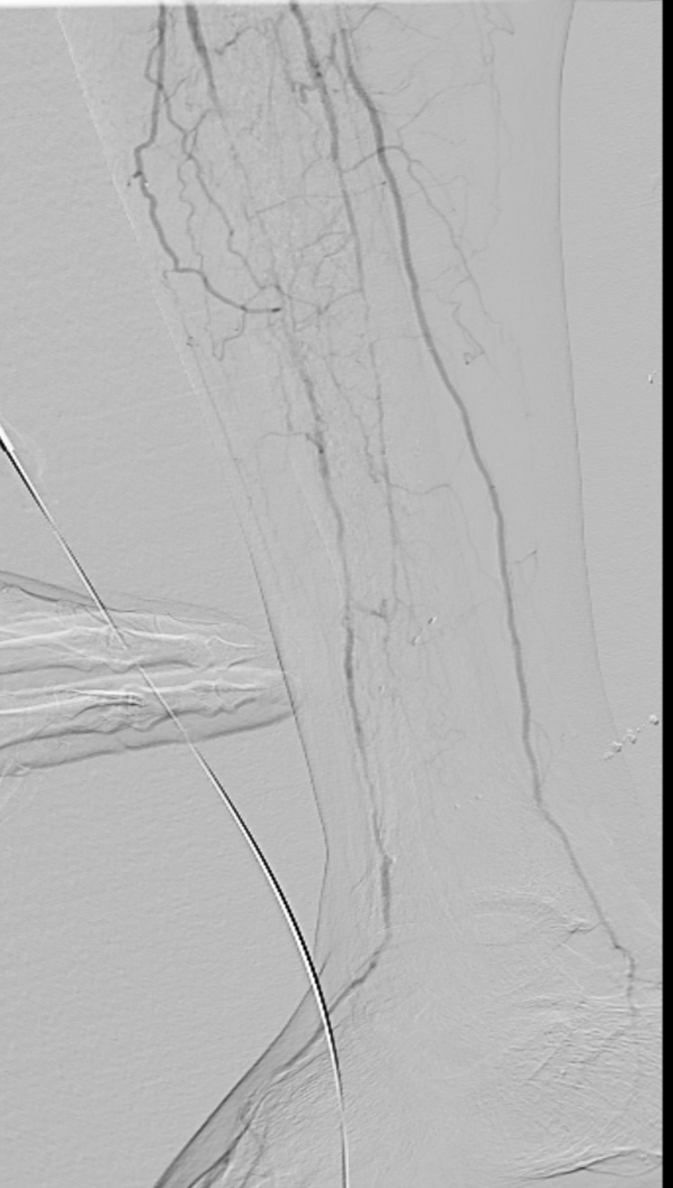
Figure 2B. Preintervention mid-AT artery occlusion (A) and DPA occlusion (B).



Next, the AT artery was cannulated with a combination of an 0.018-inch, 150-cm NaviCross support catheter (Terumo Interventional Systems) and a 0.014-inch Fielder XT wire (Asahi Intecc USA, Inc.). The occlusions of the AT artery and DPA were crossed, and the true lumen was confirmed distally. Next, a 2- X 220-mm Advance Serenity PTA balloon (Cook Medical) was exchanged and prolonged inflation angioplasty performed, starting from the most distal DPA in the foot into the AT artery (Figure 3). Significant recoil remained, with severe calcified stenosis predominately at the distal AT artery near the bend of the ankle into the proximal DPA. A 2.5- X 80-mm Serranator was advanced, with overlapping 2-minute inflations to a maximum of 6 atm with full expansion (Figure 3). This same balloon was used to perform prolonged inflation angioplasty to the previously occluded mid segment of the AT artery.
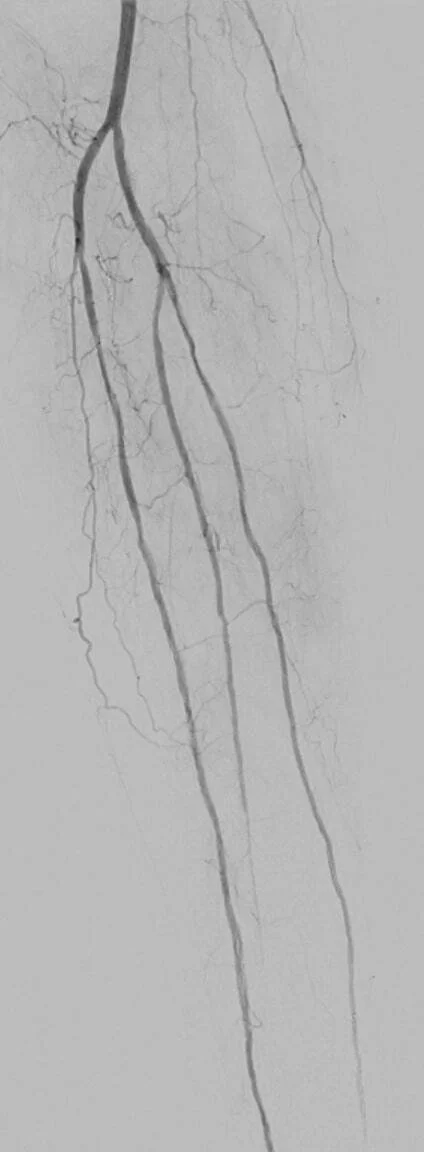
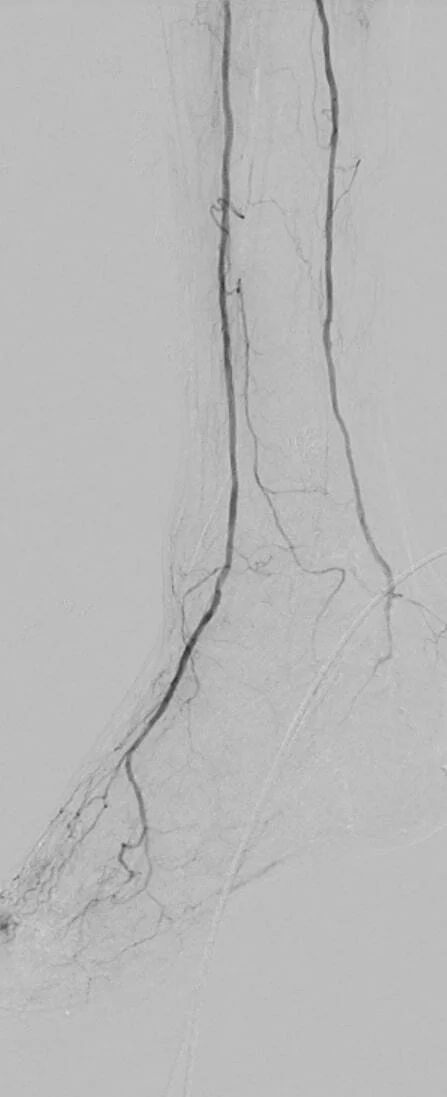
Attention turned to the PT artery and TPT. Using the 0.018-inch NaviCross catheter and 0.014-inch Fielder XT wire, the heavily diseased TPT and PT artery were subsequently cannulated. To achieve improved luminal gain prior to angioplasty, the decision was made to perform directional atherectomy of the TPT and proximal PT artery using the Pantheris device (Avinger, Inc.). After multiple passes, good luminal gain was achieved. Optical coherence tomography (OCT) was used to size the vessels, followed by a 3.5- X 40-mm Serranator for angioplasty up to a maximum of 6 atm with full expansion for 2 minutes (Figure 4). Finally, the previous 2.5- X 120-mm Serranator was used for inflation angioplasty to the PT artery down to the level of the takeoff of the plantar vessels. Completion angiogram revealed brisk two-vessel runoff with wound blush identified (Figure 5).
POSTINTERVENTION
The next day, a revision of his fifth toe amputation site was performed down to the level of the metatarsal, completing a full fifth-toe ray amputation. The wound was irrigated, and the overlying tissue layer was closed. Sterile compressive dressings were applied. The patient presented 1 month later with a healed amputation site after strict nonweight-bearing protocol to his right foot and 6 weeks of intravenous antibiotic therapy (Figure 6).

DISCUSSION
Why have you added Serranator to your BTK algorithm?
We’ve historically not had great treatment options for BTK and limited bailout options when complications arise. I feel the Serranator allows the safest and most effective way to improve luminal gain and distal perfusion in these fragile vessels. It also decreases the need for post–balloon scaffold placement BTK, which I believe is the best outcome for the patient.
How often do you experience recoil with a plain balloon versus Serranator?
This is where I believe you see the true benefit of serration technology. In complex CLTI patients, you can expect restenosis and recoil and sometimes multiple interventions. Recoil and restenosis following POBA remain unfortunately common. Since starting use of Serranator balloons, the amount of recoil and restenosis I have seen has significantly declined. This was shown in the recent RECOIL study, which compared measured recoil in Serranator- and POBA-treated lesions.
What type of results do you typically see when using the Serranator?
As mentioned, the amount of recoil and restenosis in the BTK vessels has reduced significantly. The results have been excellent in terms of prolonging patency, and more importantly, healing of wounds.