Case StudiesSerranator Use in BTK
Daniel Leung, MD, FSIR and Trelawny Zimmermann, DO | Christiana Care, Newark, DE
PATIENT PRESENTATION
A man in his mid-50s presented with a nonhealing right fifth toe amputation site. His risk factors included active smoking, diabetes, end-stage renal disease, hyperlipidemia, and atrial fibrillation. He is maintained on 75 mg clopidogrel once daily and 5 mg apixaban twice daily. Noninvasive studies demonstrated patent femoropopliteal outflow with blunted ankle waveforms and noncompressible ankle-brachial indices (ABIs).
INTERVENTION
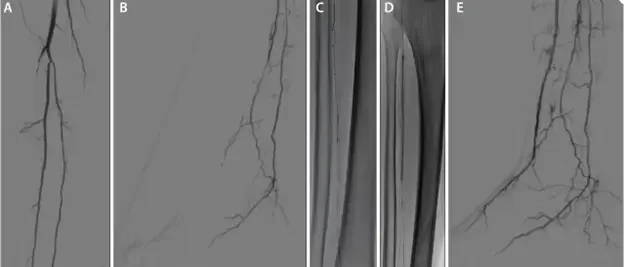
The procedure began with antegrade common femoral artery access with a 6-F, 25-cm sheath. Arteriography demonstrated patent peroneal and posterior tibial arteries with a long-segment chronic total occlusion (CTO) of the anterior tibial (AT) artery, which could not be recanalized from an antegrade approach (Figure 1A). There was a lack of flow in the dorsalis pedis (DP) artery to supply the target angiosome (Figure 1B). Retrograde access was achieved through a hibernating distal DP to facilitate AT recanalization using the subintimal arterial flossing with antegrade-retrograde intervention (SAFARI) technique (Figured 1C). After predilation with a 2- X 40-mm balloon, a 3- X 120-mm Serranator PTA balloon was inflated slowly to 6 atm for 2 minutes over several stations from the DP to the proximal AT (Figure 1D). Completion arteriography demonstrated a widely patent AT and DP with perfusion to the target digit five wound bed (Figure 1E).
CONCLUSIONS
The Serranator balloon was perfectly suited to augment long-segment AT recanalization, achieving impressive luminal gain and brisk flow to the lateral forefoot wound. The patient went on to heal his minor amputation site wound in 6 weeks.