
Case StudiesHealing That Lasts
Real-World 90-Day Outcomes Demonstrating the Durability of Serration Remodeling Therapy (SRT)
Sagar S. Gandhi, MD | Prisma Health, Greenville, SC
Introduction
Tibial arterial disease remains one of the most challenging areas in peripheral intervention. Patients often present with critical limb ischemia, nonhealing wounds, prior amputations, long-segment occlusions, heavy calcification, and small-caliber vessels. These factors limit procedural success and contribute to high rates of recoil, restenosis, and reintervention.
Plain balloon angioplasty (POBA) frequently fails to deliver durable tibial outcomes due to recoil and the rigidity of calcified arteries. Adjunctive options such as atherectomy or intravascular lithotripsy (IVL) may help but add procedural complexity, cost, and risk, and are not always feasible below the knee. These limitations highlight the need for approaches that achieve reliable vessel expansion without increasing procedural burden.
Serration Remodeling Therapy (SRT)
Serration Remodeling Therapy (SRT) uses low-pressure inflation to release the internal elastic lamina, reducing recoil while increasing luminal gain and volumetric flow. The Serranator’s stainless-steel serration strips focus force along the vessel wall, creating controlled micro-fractures in calcified plaque. This mechanism promotes predictable expansion at lower pressures, minimizes vessel trauma, improves compliance, and supports sustained flow in rigid, calcified segments.
Serranator’s design is well suited for tibial vessels, where small diameter and heavy calcification make treatment difficult. Its controlled expansion can reduce the need for adjunctive therapies while supporting consistent inline flow to the foot, which is critical for wound healing and limb salvage.
Methodology
This case series includes four consecutive patients with severe tibial disease presenting with nonhealing wounds, prior toe amputations, and markedly impaired perfusion. All required infrapopliteal intervention, and SRT was used as the primary treatment for the target tibial segment (device sizes 2.5–3.5 mm). Adjunctive POBA or DCB was used only when necessary and is described in individual cases.
Patients were followed at approximately 30, 60, and 90 days with clinical assessment, ABI and toe pressures when feasible, wound evaluation, and angiography when clinically indicated. Follow-up focused on vessel patency, perfusion improvement, vessel behavior over time, and wound progression.
Objective
The objective was to assess whether SRT could provide durable luminal gain in tibial vessels, where treatment options are limited and repeat interventions are common. Specifically, this series evaluated whether SRT could maintain patency long enough to support wound healing without reintervention, and whether improvements in vessel compliance translated into measurable hemodynamic and clinical outcomes. The goal was to determine whether SRT could serve as a reliable first-line tool for complex tibial limb salvage interventions.
Patient A
Presentation
A 77-year-old male presented with a great toe infection requiring amputation. Postoperatively, he exhibited poor bleeding, ischemic wound edges, and delayed healing potential. He had no palpable pedal pulses, known recurrent tibial disease, and several prior interventions. Angiography showed long-segment anterior tibial (AT) and posterior tibial (PT) stenoses and multiple focal occlusions extending distally to the foot.

Procedure
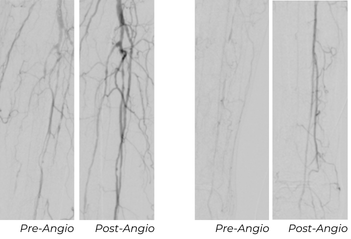
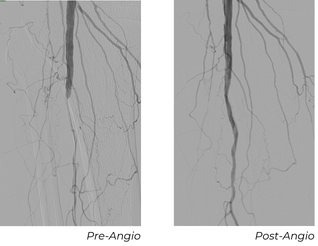
Using a 6 Fr sheath, a 0.014" Glide Advantage, and a 0.014" CXI, the vessel was predilated with a 2 mm POBA balloon to assist in delivery. A 2.5x80 mm Serranator was then used within the left AT. The posterior tibial (PT) artery was also diseased, but due to limited devices stocked, it was treated with a 2 mm POBA balloon. The result provided restoration of continuous AT flow to the foot and an initial improvement in the PT.
Follow-Up Outcomes
At this patient’s 30-day follow-up appointment, ultrasound showed the AT, which was treated with Serranator, remained fully patent. The PT, treated with POBA, had re-occluded. The wound showed robust granulation tissue and the 2 cm post-amputation cavity had nearly filled, and the ABI was 0.94.
At the 90-day follow-up appointment, ABI remained stable at 1.01, with the AT still patent without restenosis, and the PT remained occluded. The patient’s residual wound had essentially healed with only a small residual eschar.

Key Takeaway
This case illustrates significant durability of the intervention and no vessel recoil after Serration Remodeling Therapy. This enabled wound healing without reintervention through 90 days, contrasted with early PT failure after POBA.
Patient B
Presentation
A 68-year-old male patient presented with a second-toe ulcer and a history of multiple prior anterior tibial interventions. For the past 4 years, the patient had a chronic recurrent wound despite multiple successful treatments of his AT with POBA. The last 2 interventions, each failed within a few weeks. Non-invasive testing showed a heavily calcified ABI at 1.7 and a toe pressure of 32 mmHg.
Procedure
A 5 Fr sheath was placed in the below-knee popliteal artery. Selective angiogram of the AT artery again demonstrated the long segment occlusion. Using an 0.018" glide advantage wire and CXI catheter we were able to select the AT. Once the occlusion was traversed, the wire was exchanged for an .014” Roadrunner wire. We performed predilation of the occlusion with a 1.5x40 mm POBA followed by 2.5x100 mm POBA. Next, we performed Serration Remodeling Therapy with the 3.0x80 mm Serranator. Completion angiogram demonstrated complete resolution of the occlusion and excellent flow into the foot.

Follow-Up Outcomes
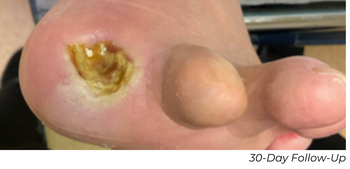
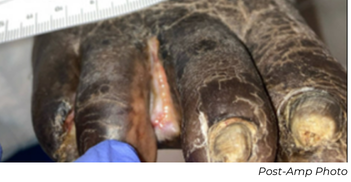
Before his 30-day follow-up appointment, the patient had undergone a previously planned first toe amputation for osteomyelitis. At 30-day follow-up appointment for the amputation, the patient still had a calcified ABI at 1.6, but the toe pressure increased to 101 mmHg. The post-amputation wound showed substantial improvement as well. At the 60-day follow-up appointment, his ABI was normalized to 1.29, the toe pressure was still maintained at 112 mmHg, and his wound was healed.
Key Takeaway
This case demonstrates restored vessel compliance, normalization of ABI, and a striking increase in toe pressure following Serration Remodeling Therapy, supporting sustained perfusion and complete wound healing.
Patient C
Presentation
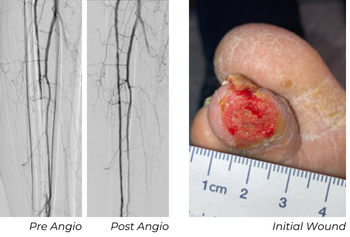
A 72-year-old male with a third toe amputation presented from the wound care center with stalled wound healing. He had a calcified ABI at 1.64 and critically low toe pressure of 9 mmHg. His amputation site wound was present for 6 months with minimal progress. Images of the right lower extremity were obtained which showed the tibioperoneal trunk (TPT) was occluded but the peroneal artery filled via geniculate collaterals and was the only runoff down to the foot.
Procedure
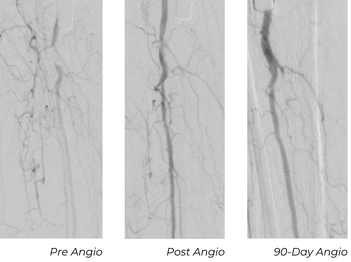
A 5 Fr sheath was inserted with a 0.014” glide advantage wire. We were able to cross the TPT occlusion and performed Serration Remodeling Therapy with a 3.0x80 mm Serranator. Completion imaging showed no dissection, spasm, or thrombus, but there was residual stenosis at the ostium of the TPT. A 3.5x20 mm Serenity® PTA Balloon was used to perform angioplasty.
Follow-Up Outcomes
At his 30-day follow-up appointment, the wound was significantly smaller with healthy tissue formation, measuring 0.8x0.3 cm, down from the original wound size of 1x0.5 cm. At the 90-day follow-up appointment, his ABI was normalized at 0.93 and his toe pressure improved to 33 mmHg.

Key Takeaway
This case highlights progressive vessel remodeling after Serration Remodeling Therapy, continued luminal improvement, normalization of perfusion metrics, and complete wound healing within 90 days.
Patient D
Presentation
An 89-year-old male presented with a right great toe wound complicated by osteomyelitis. A right lower extremity angiogram was performed which showed the TPT high-grade 90% stenosis with the peroneal as the only runoff to the foot.
Procedure
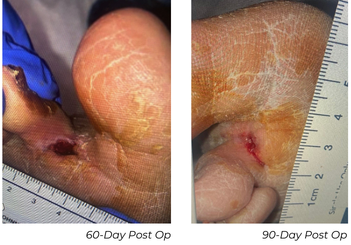
A 5 Fr sheath was inserted with a 0.014” glide advantage wire. We were to traverse the stenotic segments and used a 3.5x80 mm Serranator followed by 4.0x60 mm DCB. Intravascular ultrasound confirmed no residual stenosis. There was brisk flow down to the foot via the peroneal. The immediate result was an ABI of 0.99 and a toe pressure of 58 mmHg.

Follow-Up Outcomes
This patient needed a toe amputation one month after his procedure due to osteomyelitis. After one-month, the patient had wound dehiscence, therefore a repeat angiogram was performed. Repeat imaging showed excellent remodeling, no restenosis, and a strong, in-line flow. The wound has progressed significantly, and the patient is near healed.

Key Takeaway
Despite this patient’s advanced age and wound complications, the TPT vessel demonstrated durable patency and positive remodeling after Serranator use, with no need for repeat angioplasty.
Case Series
Consolidated Findings
Across four patients treated for tibial disease, consistent clinical signals emerged. All Serranator-treated vessels remained patent through 90 days, with no repeat angioplasty or adjunctive reintervention required. Durable luminal gain was achieved even in heavily calcified vessels and long-segment occlusions. Toe pressures increased in all cases, and previously noncompressible ABIs normalized by 60–90 days in multiple patients, suggesting improved vessel compliance beyond the immediate procedural effect.
Wound healing paralleled these findings. All patients showed progressive tissue recovery, from early granulation at 30 days to near or complete closure by 90 days. When follow-up imaging was obtained, 90-day angiograms were often equal to or better than completion angiograms, indicating ongoing positive remodeling. In one comparison, a PT treated with POBA alone re-occluded within 30 days, while the Serranator-treated AT remained patent, highlighting recoil suppression.
Collectively, the series demonstrates durable patency, improved compliance, enhanced perfusion, and meaningful wound healing without repeat intervention, suggesting Serranator may serve as a reliable first-line mechanical option for complex tibial disease.
Discussion
The durability of luminal gain observed with Serration Remodeling Therapy appears linked to the mechanical design of Serranator. Stainless-steel serration strips create a focused force profile that produces predictable plaque fracture at lower pressures, potentially reducing elastic recoil compared with conventional POBA, a key advantage in calcified tibial vessels where recoil drives restenosis.
Sustained luminal stability also appeared to influence wound healing. In patients with tissue loss, even modest improvements in tibial patency can significantly impact foot perfusion. Achieving immediate, stable expansion with limited vessel trauma may support more reliable microvascular recovery.
These findings are limited by small sample size and single-center experience. Larger studies, longer follow-up, and broader patient cohorts are needed. A tibial-focused registry and comparative studies versus POBA would help clarify the specific role of Serration Remodeling Therapy in recoil reduction and long-term patency. These early observations, however, help inform where SRT may fit within evolving tibial treatment strategies.
Conclusion
This case series highlights the potential of Serration Remodeling Therapy in complex tibial artery disease, where durable perfusion is critical for wound healing. Across four patients, Serranator achieved controlled luminal gain with minimal trauma, no early recoil, and sustained results through 90 days, without the need for reintervention.
Although limited by size and scope, these findings provide early evidence that SRT may address a major gap in tibial therapy. Further study is warranted, but this experience suggests improved limb salvage outcomes, may be achievable with Serration Remodeling Therapy.
