
Case StudiesUse of SRT Technology in common Iliac Artery Stenosis
Neil Poulsen, MD | Clara Maass Medical Center Belleville, New Jersey
Introduction
My patient is a 58-year-old female with a complex medical history including type II diabetes, chronic kidney disease, hypertension, peripheral vascular disease, and coronary artery disease. She presented with left foot gangrene and dehiscence of a previous left toe amputation site.
During angiography, I identified a significant stenosis in the right common iliac artery, located at the aortic bifurcation. This presented a treatment challenge: placing a stent would require bilateral (“kissing”) stents, effectively raising the bifurcation and limiting future access options for interventions on the left side, which was her primary problem. Although the right-sided lesion was incidental, it needed to be treated to improve overall perfusion and maintain access for future procedures.
Treatment
To avoid stenting at the bifurcation, I selected the Serranator Serration Balloon Catheter. The availability of larger balloon sizes and the ability to achieve effective dilation at low atmospheric pressure made it an ideal choice for this anatomy.
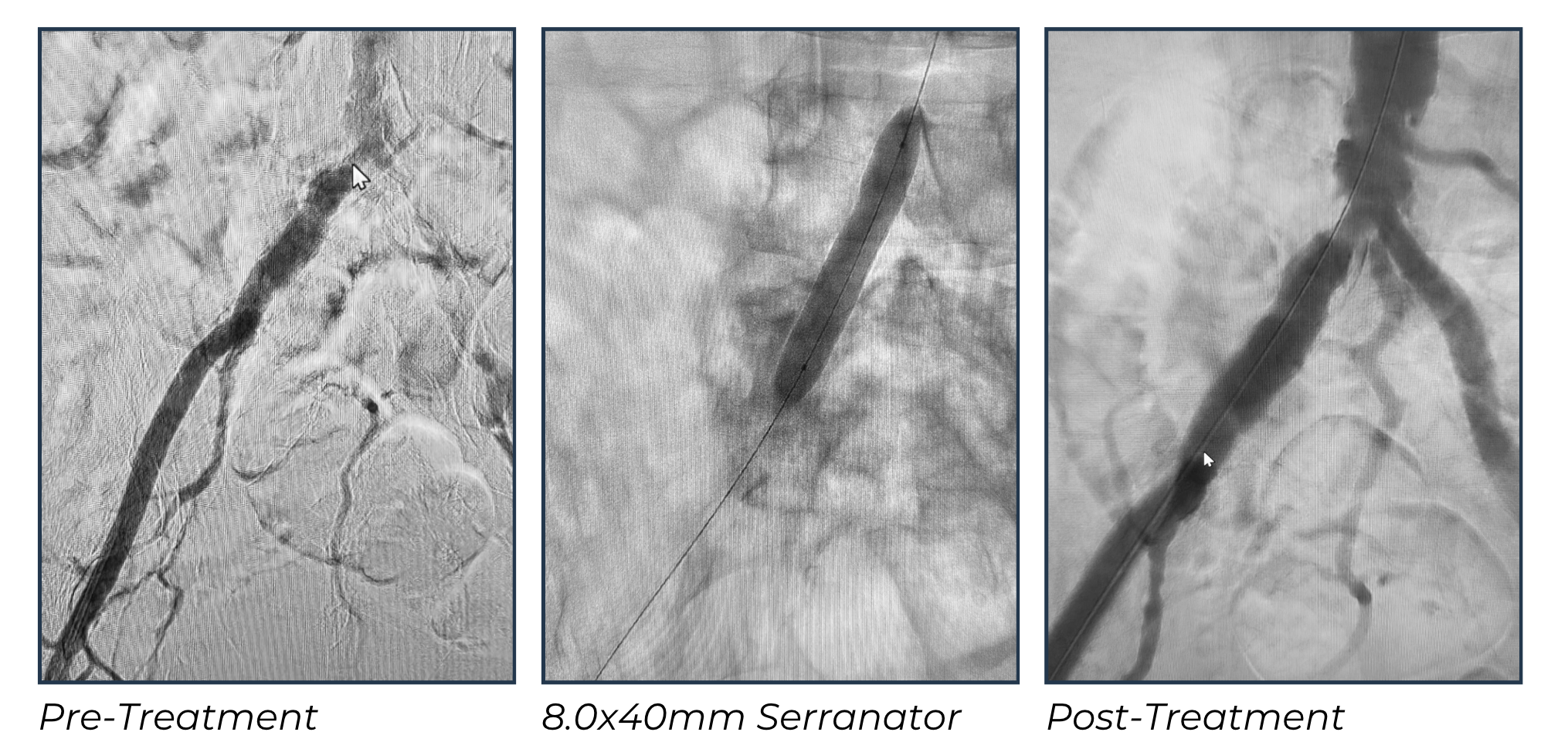
Using an 8.0x40mm Serranator, I was able to treat the lesion with precision and control. The serration technology provided effective luminal expansion while minimizing the risks of dissection and rupture that are commonly associated with POBA.
The procedure was straightforward, with a visible waist on the balloon during inflation that resolved completely at 4 atmospheres of pressure. The technology allowed me to achieve an excellent angiographic result without the need for stent placement. For me, this was a low-risk, high-reward approach that preserved vessel integrity and kept future treatment options open.
Given the patient’s previous interventions and diffuse disease, I was particularly pleased to avoid stenting at the bifurcation. A kissing stent would have raised the bifurcation and restricted the ability to go up and over in future procedures, which would have been problematic for her ongoing care.
Outcome
The angiographic results were excellent. The initial image showed a severe stenosis at the right common iliac bifurcation, which resolved completely following Serranator inflation. The final angiogram demonstrated near-complete resolution of the lesion and improved flow to the right leg. No dissection, rupture, or other complications occurred. The procedure was efficient, safe, and provided durable results without the use of a stent.
Final Thoughts
This case highlights the value of Serranator’s Serration Technology in complex bifurcation lesions where maintaining access for future interventions is critical. Serranator allowed me to achieve excellent luminal gain at low pressure, without compromising vessel integrity or limiting future treatment options. Serranator provided a safe, predictable, and effective solution in a challenging anatomic location, making it a valuable tool in my endovascular practice.