
Serration Remodeling Therapy
A fundamentally different approach to peripheral intervention built on physics, proven in clinical practice.
Conventional balloon angioplasty works by stretching the arterial wall.
That uncontrolled stretch is also its limitation: high recoil rates, unpredictable dissection, and the frequent need for bailout stenting.

Serration Remodeling Therapy takes a different approach.
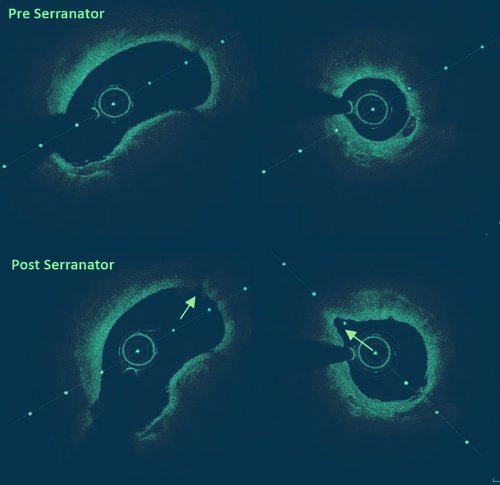
By concentrating force into precise contact points along the vessel wall, SRT creates a controlled line of weakness in the lesion, opening the artery predictably at low pressure, without the trauma of overinflation.
The result is consistent lumen gain, minimized recoil, and a dramatically lower stent rate across all lesion morphologies.
The Physics Behind SRT
Serration Technology: Physics Put to Work
Serration technology isn’t new, it’s a fundamental principle of physics applied across automotive, construction, and aviation industries. Small, concentrated points of contact apply exponentially greater pressure per unit area than a flat surface. The linear line that results is more responsive to directed energy and opens more predictably than a surface under distributed load.
The Serranator applies this same principle inside the vessel. Its stainless-steel serration strips are bonded along the balloon surface. At low inflation pressures, these strips concentrate force into precise contact points against the arterial wall, applying 1,000× the point force of a plain angioplasty balloon. The result is a controlled serration line that opens the lesion predictably, without the circumferential stretch that drives recoil and dissection.
-
Point Force
Concentrated force at each serration point
-
Stainless-Steel Serration Strips
Bonded strips apply precise, repeatable pressure along the balloon surface
-
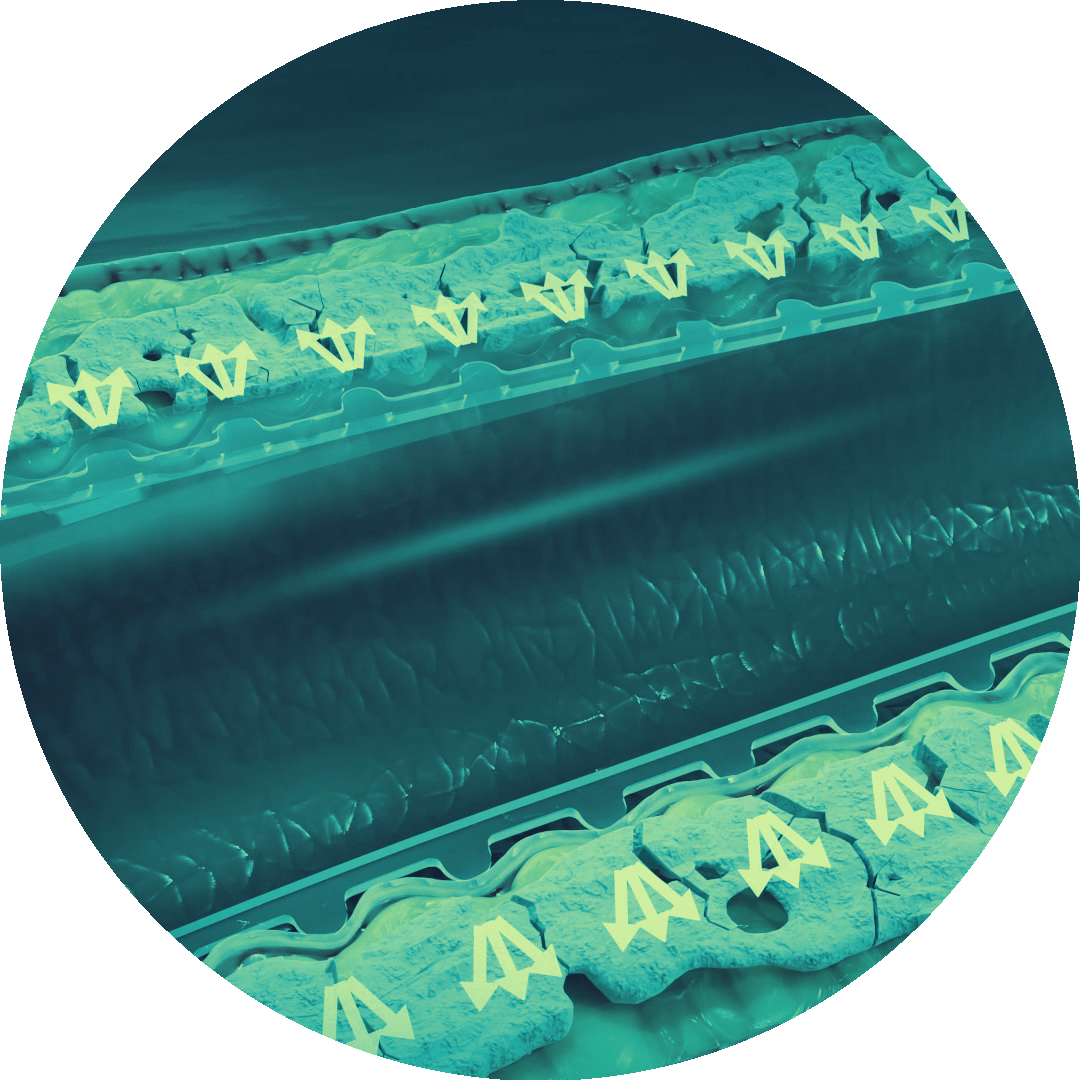
MOA cross-section
Arterial expansion follows the serration line effective across all lesion morphologies
Why SRT Changes Outcomes in PAD
The limitations of plain balloon angioplasty are not incidental, they are mechanical. Circumferential stretch creates unpredictable dissection planes and elastic recoil that erodes lumen gain within minutes of deflation. Serration Remodeling Therapy addresses each of these failure modes at the mechanism level.
Key Benefits
Internal elastic lamina disruption: controlled release of the IEL along the serration line, not random tearing
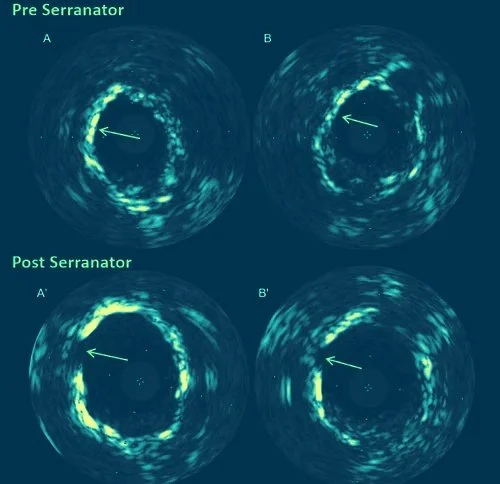
Reduced recoil mechanics: 89% less average recoil than POBA, sustained at follow-up
Controlled serration vs. uncontrolled stretch: predictable lesion yield across calcified, fibrotic, and mixed morphologies
Low-pressure remodeling: effective lumen gain without the overinflation that drives dissection

SRT vs. Traditional Angioplasty:
A Fundamental Difference
Plain balloon angioplasty stretches the vessel wall in all directions, creating an uncontrolled failure plane that varies with lesion composition, calcification burden, and inflation pressure. SRT replaces that mechanism with directed point-force serration: a repeatable, low-pressure process that produces consistent results regardless of lesion morphology.
| POBA | SRT | |
|---|---|---|
| Mechanism | Circumferential stretch | Controlled point-force serration |
| Recoil | High (55% average) | Low (6% average) |
| Dissection risk | Unpredictable | Minimized via controlled serration line |
| Inflation pressure required | 9ATM average | 5ATM average |
| Lesion morphology coverage | Limited efficacy in calcification | Effective across all morphologies |
Effective In All Lesion Morphologies
One of the most clinically meaningful advantages of SRT is its consistency across lesion types. Where plain balloon angioplasty is most prone to failure in heavily calcified or fibrotic lesions, precisely the anatomy that defines complex PAD, the Serranator’s serration mechanism is not dependent on lesion compliance.
The serration line follows the physics of concentrated point force, not the mechanical properties of the tissue. This means predictable lumen gain whether the operator is treating a soft, fibrous lesion in the SFA or a heavily calcified tibial vessel in a CLTI patient.
-
Calcified
Concentrated point force penetrates where POBA stretch fails
-
Fibrotic
Controlled serration without unpredictable dissection planes
-

Soft / lipid-rich
Low-pressure SRT avoids overinflation and vessel trauma
-
Mixed morphology
Consistent yield regardless of composition variability
-

Long lesions
Serration line extends along balloon length for uniform treatment
our products
Choose the Right Tool for Your Patient
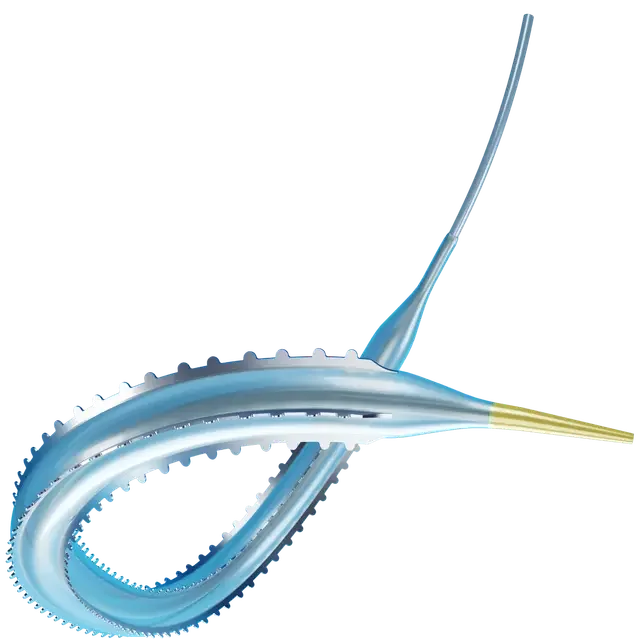
THE SERRANATOR
For ATK, BTK, and fistula anatomy, a comprehensive size range from 2.5–8.0 mm across SFA, popliteal, tibial, and dialysis access applications.
Explore the Serranator
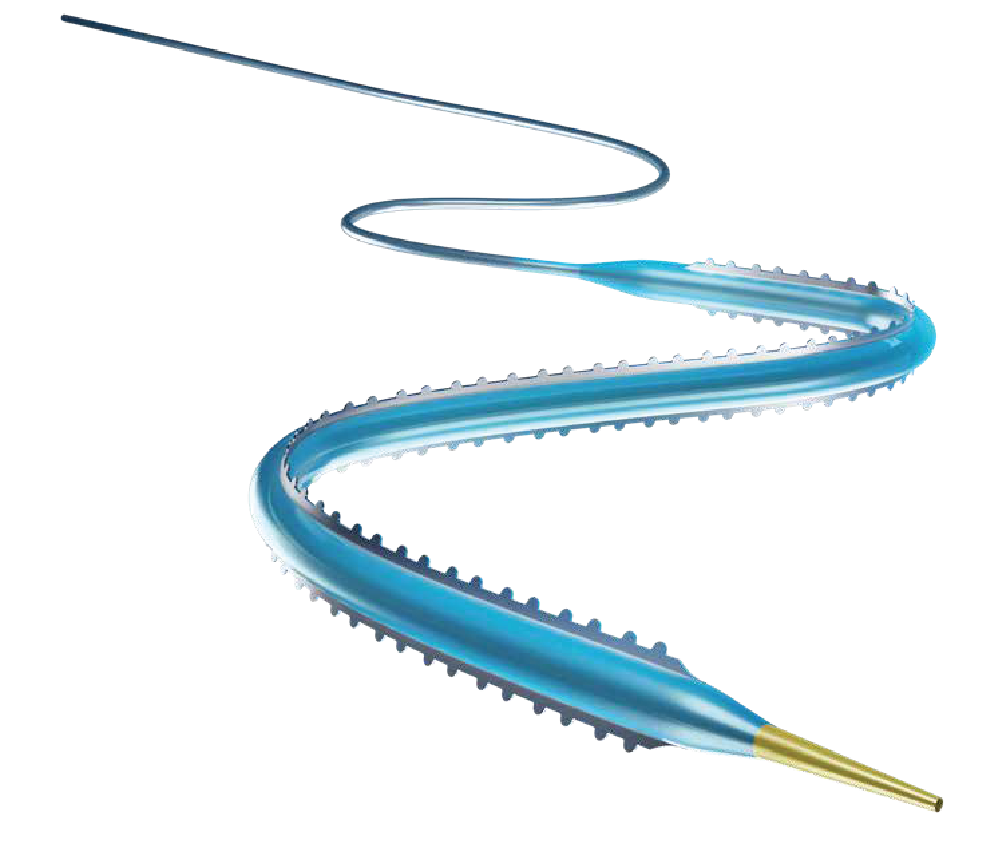
THE SERRANATOR SL-PRO
Purpose-built for pedal and CLTI disease, 5F compatible, 2.0 mm, 60% more trackable for distal anatomy where outcomes matter most.
Explore the Serranator SL-PRO
The Evidence Behind SRT
Serration Remodeling Therapy is backed by a growing body of clinical evidence across multiple studies, lesion types, and anatomic territories. From PRELUDE to RECOIL, the data consistently demonstrates superiority over plain balloon angioplasty on the metrics that matter most: patency, recoil, and stent avoidance.

Ready for SRT to address your current challenges?
Data provided by
Guetl K, Muster V, Schweiger L, Tang WC, Patel K, Brodmann M. Standard Balloon Angioplasty Versus Serranator Serration Balloon Angioplasty for the Treatment of Below-the-Knee Artery Occlusive Disease: A Single-Center Subanalysis From the PRELUDE-BTK Prospective Study. J Endovasc Ther. 2024 Aug;31(4):615-621. doi: 10.1177/15266028221134891. Epub 2022 Nov 20. PMID: 36408609.
Fereydooni A, Chandra V, Schneider PA, Giasolli R, Lichtenberg M, Stahlhoff S. Serration Angioplasty Is Associated With Less Recoil in Infrapopliteal Arteries Compared With Plain Balloon Angioplasty. J Endovasc Ther. 2025 Oct;32(5):1600-1606. doi: 10.1177/15266028231215284. Epub 2023 Dec 7. PMID: 38059463.
Fanelli F, Cannavale A, Gazzetti M, Lucatelli P, Wlderk A, Cirelli C, d'Adamo A, Salvatori FM. Calcium burden assessment and impact on drug-eluting balloons in peripheral arterial disease. Cardiovasc Intervent Radiol. 2014 Aug;37(4):898-907. doi: 10.1007/s00270-014-0904-3. Epub 2014 May 9. PMID: 24806955.
Holden A, Lichtenberg M, Nowakowski P, Wissgott C, Hertting K, Brodmann M. Prospective Study of Serration Angioplasty in the Infrapopliteal Arteries Using the Serranator Device: PRELUDE BTK Study. J Endovasc Ther. 2022 Aug;29(4):586-593. doi: 10.1177/15266028211059917. Epub 2021 Nov 20. PMID: 34802313.